Research Week 2022 – Emily Mann, MD
Culture Negative Endocarditis and Recurrent Fevers
Emily Mann
Learning Objectives
- Recognize a common Q fever endocarditis presentation
- Define persistent focal Q fever
- Understanding the importance of lymphadenopathy in the setting of Q fever
A 40 year old male with a past medical history of rheumatic heart disease presented to
his primary care doctor for two years of worsening, intermittent fevers.
The patient had lived all over the world, including various parts of Africa and Europe. He
took no medications and used no illicit drugs. He worked in construction and lived in the
suburbs of Massachusetts with his family. He had no pets. His only exposure to
livestock was about three years prior to presentation at a fair.
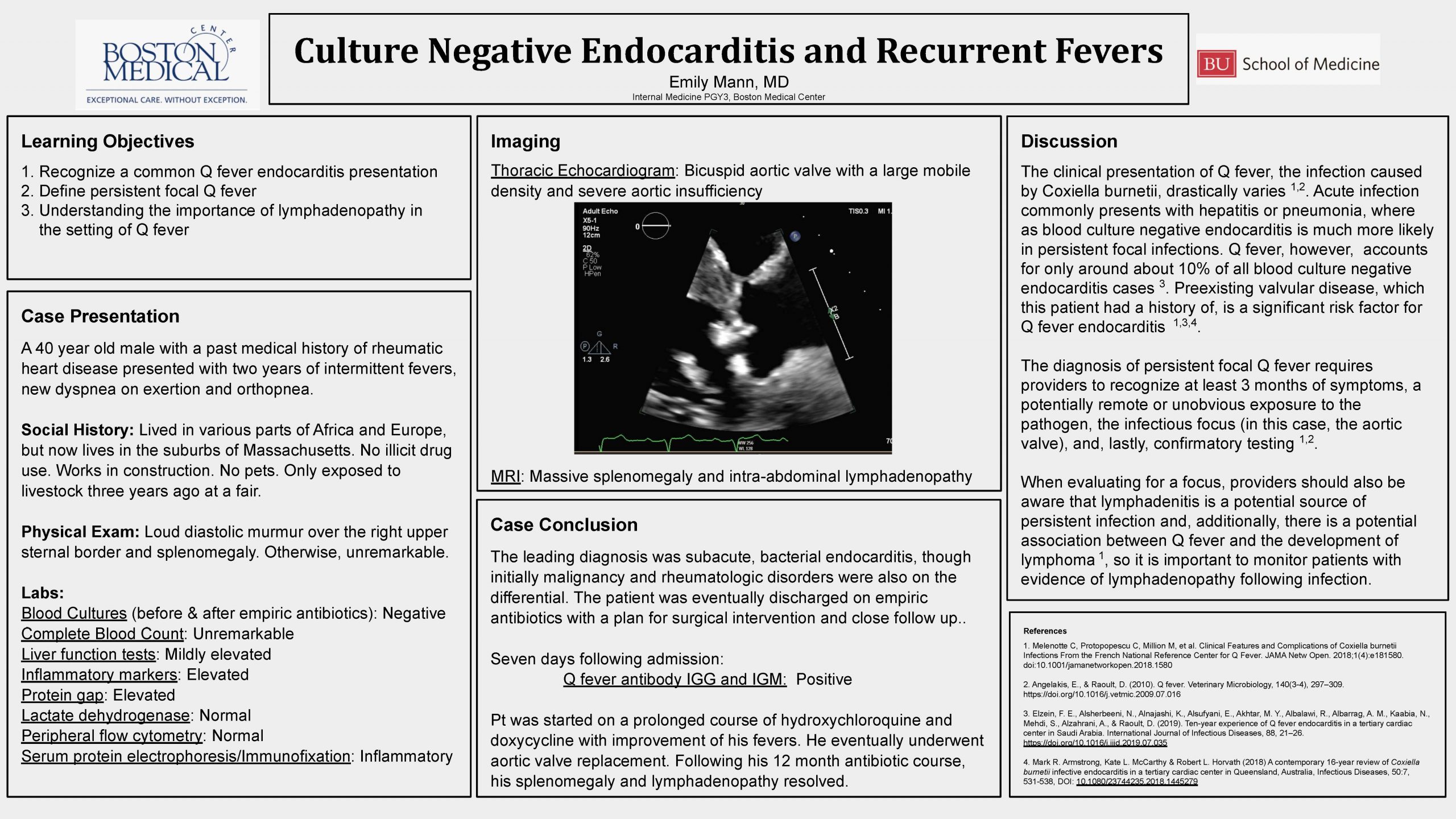
Over the course of his evaluation for fevers, he began to have dyspnea on exertion and
orthopnea, so he underwent transthoracic echocardiogram. The echocardiogram
revealed a bicuspid aortic valve with a large mobile density and severe aortic
insufficiency, so he was admitted to the hospital for further work up.
Blood cultures were drawn prior to initiation of antibiotics and were negative. Labs were
significant for a normal white blood count and differential, mild anemia, normal platelets,
mildly elevated liver function tests, elevated inflammatory markers and an elevated
protein gap. MRI revealed massive splenomegaly and intra-abdominal
lymphadenopathy. Physical exam was significant only for a loud diastolic murmur over
the right upper sternal border and splenomegaly. Concern was primarily for subacute,
bacterial endocarditis, though the differential included malignancy and rheumatologic
disorders.
Repeat blood cultures throughout the admission were negative, but empiric antibiotics
were started. Lactate dehydrogenase was within normal limits. Peripheral flow
cytometry was normal. Serum protein electrophoresis and immunofixation suggested
only generalized inflammation. Seven days following admission, his Q fever antibody
IGG and IGM returned positive and he was started on a prolonged course of
hydroxychloroquine and doxycycline with improvement of his fevers. He eventually
underwent aortic valve replacement and, following his 12 month antibiotic course, his
splenomegaly and lymphadenopathy resolved.
Despite this patient’s chronic fevers and endocarditis being classic features of persistent
focal Q fever, it was not highest on the differential. The clinical presentation of Q fever
varies significantly and this case demonstrates the importance of keeping Q fever on
the differential even when acute exposure is not obvious.
References
- Melenotte C, Protopopescu C, Million M, et al. Clinical Features and Complications of
Coxiella burnetii Infections From the French National Reference Center for Q Fever.
JAMA Netw Open. 2018;1(4):e181580. doi:10.1001/jamanetworkopen.2018.1580
- Angelakis, E., & Raoult, D. (2010). Q fever. Veterinary Microbiology, 140(3-4),
297–309. https://doi.org/10.1016/j.vetmic.2009.07.016
- Elzein, F. E., Alsherbeeni, N., Alnajashi, K., Alsufyani, E., Akhtar, M. Y., Albalawi, R.,
Albarrag, A. M., Kaabia, N., Mehdi, S., Alzahrani, A., & Raoult, D. (2019). Ten-year
experience of Q fever endocarditis in a tertiary cardiac center in Saudi Arabia.
International Journal of Infectious Diseases, 88, 21–26.
https://doi.org/10.1016/j.ijid.2019.07.035
- Mark R. Armstrong, Kate L. McCarthy & Robert L. Horvath (2018) A contemporary
16-year review of Coxiella burnetii infective endocarditis in a tertiary cardiac center in
Queensland, Australia, Infectious Diseases, 50:7, 531-538, DOI:
10.1080/23744235.2018.1445279